
| Teaching Round | |
| A Young Man with Cough, Eosinophilia and Pulmonary Infiltrates | |
| Ghan Shyam Pangtey*, Randeep Guleria**
**Lady Hardinge Medical College and associated hospitals, New Delhi.
** All India Institute of Medical Sciences, New Delhi. Corresponding Author: Dr Ghan Shyam Pangtey, Assistant Professor, Dept. of Medicine, LHMC and associated hospital, Delhi. Email: drpangtey@yahoo.com
Twenty six year old non smoker male, resident of Haryana (India), was admitted for elective surgery. Medical consultation for pre-anaesthetic clearance before surgery was sought for respiratory symptoms. Patient complained of dry cough, breathlessness on exertion and wheezing for the past two weeks. It was not associated with any fever, nasal discharge, sore throat. There was no previous history of similar episode of wheezing chronic cough or dyspnoea. On examination his vitals were stable and systemic examination was remarkable for the presence of bilateral extensive inpiratory and expiratory wheeze with prolonged expiration. Preoperative investigations revealed hemoglobin of 3 14 gm/dL; leukocyte count 47,800/ mm3 with 75% eosinophils, 15% polymorphs, 10% lymphocytes. His erythrocyte sedimentation rate was 40 mm at the end of first hour. Liver as well as kidney function tests were in normal range.  Patient was further investigated for eosinophilia and chest findings. Stool examination for ova and cyst was negative and peripheral smear for Microfilaria was unrevealing; there was no evidence of immature or abnormal cells on peripheral blood smear. His serum Angiotension Converting Enzyme (ACE) levels and urinary calcium were normal. High resolution CT (HRCT) and CECT chest was done (Figure 2). 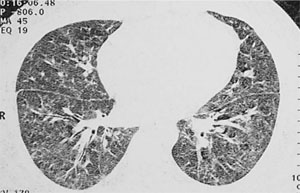 What are the chest X ray and HRCT findings? Chest X ray PA view reveals bilateral lower zone haziness with small reticulonodular opacities. HRCT confirms the finding of reticulonodular shadow and ground glass haziness in bilateral lung fields. What is the differential diagnosis for this case? The differential diagnosis of the case with pulmonary eosinophilia is very wide and ranges from intestinal infestation with parasites (Ascaris, Toxocara, Capillaria, Schistosoma, Strongyloides, Echinococci and non-parasitic causes such as allergic bronchopulmonary aspergillosis (ABPA), extrinsic bronchial asthma, hypereosinophilic syndrome, acute eosinophilic pneumonia, sarcoidosis and tropical pulmonary eosinophilia [1]. What is the diagnosis? Tropical pulmonary eosinophilia (TPE). It is an endemic disease of tropics and is believed to be due to abnormal hypersensitivity response to filarial parasite (Wuchereria bancrofti and Brugia malayi) [2]. In persons susceptible to the development of TPE, the microfilariae released into the circulation from adult worms in the lymphatics are rapidly opsonized with antifilarial antibodies and these are then cleared in the pulmonary vasculature [3]. What are the clinical features of TPE? How can one diagnose a case of TPE? TPE occurs in <1% of patients suffering from Lymphatic filariasis. The main features include residence or travel to filarial-endemic region and symptoms of paroxysmal cough with scanty sputum, night time symptoms of wheeze, low grade fever and reticulonodular infiltrates on chest x ray. The four important criteria routinely used for diagnosis include extreme peripheral blood eosinophilia 3 (>3000/mm ), antibodies (IgG/IgE) against filarial antigen, raised IgE levels and absence of microfilariae in both day and night blood samples using concentration techniques [4]. The final criteria commonly used for the diagnosis is the dramatic response to Diethylcarbamazine (DEC), although there are a proportion of patients who do not respond to this, therefore it is not considered to be an essential criteria [5]. Clinical course and discussion The diagnosis of TPE was made after Filarial Antibody Test (FAT) was found to be positive and patient fulfilled most of the proposed criteria. He was treated with Diethylcarbamazine (DEC) 300mg/day in three divided doses for three weeks. Post-treatment he showed complete recovery with symptomatic relief in cough, dyspnoea and complete radiological resolution of mottling and reticular-nodules as well as disappearance of eosinophilia from blood. Delayed diagnosis or untreated cases of TPE can have persistent symptoms for years and may develop pulmonary interstitial fibrosis and permanent pulmonary insufficiency and damage. Computed Tomography especially HRCT has been found to be better than plain radiography in detecting nodularity, fibrosis, bronchiectasis, air trapping, mediastinal adenopathy and calcification [6]. References
|