Shilpi Gupta Dixit, Veena Bharihoke
Department of Anatomy, University College of Medical Sciences, Delhi - 110 095.
Corresponding Author: Dr. Shilpi G. Dixit, House No. 3164, Sector 23, Gurgaon-122017, Haryana
Email: shilpidr@gmail.com

Figure 1—
- Identify the region
- Identify the marked structures
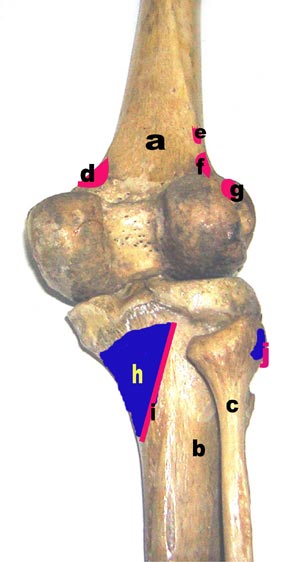
Figure 2—
- Identify the marked structures
Answers to regional anatomy at a glance
Figure 1—
- Popliteal fossa
a. Semimembranosus
b.
Semitendinosus
c.
Biceps femoris
d.
Fascia
e.
Gracilis
f.
Medial head of gastrocnemius
g.
Lateral head of gastrocnemius
h.
Popliteal artery
i.
Sciatic nerve
j.
Tibial nerve
k.
Common peroneal nerve
l.
Sural nerve
m.
Medial genicular artery
n.
Lateral genicular artery
Figure 2—
- Posterior aspect of bones in the popliteal region :
a. femur
b.
tibia
c.
fibula
d.
Origin of medial head of gastrocnemius
e.
origin of plantaris
f.
origin of lateral head of gastrocnemius
g.
origin of popliteus
h.
insertion of popliteus
i.
origin of soleus
j.
insertion of biceps femoris
Key points to remember:
- Popliteal fossa Is a diamond shaped (quadrangular) space bounded
- Superiorly- laterally, biceps femoris and medially, semimembranosus & semitendinosus.
- Inferiorly- laterally by lateral head of gastrocnemius and plantaris, while medially by medial head of gastrocnemius
- Floor: Popliteal surface of femur, oblique popletial ligament, posterior aspect of proximal tibia, fascia covering the popliteus
- Roof: Popliteal fascia. Short saphenous vein and sural nerve
- Contents of popliteal fossa— Popliteal vein (V) and artery (A) with branches, and 2 nerves (N) tibial and common peroneal with their branches
- Relations of contents
Upper part—AVN --from medial to lateral
Middle part—AVN --from anterior to posterior
Lower part—NVA -- from medial to lateral
| • |
Secondary ossification centre of lower end of femur appears at 9th month of intrauterine life. Presence indicates viable birth. |
| • |
The capsule of knee joint is attached proximal to the epiphyseal line thus joint is spared of osteomyelitis. |
| • |
Common peroneal nerve winds around neck of fibula thus lesions at this region lead to injury of the nerve resulting in foot drop and loss of inversion with sensory loss on anterolateral aspect of leg and dorsum of foot. |
| • |
Tibial nerve injury due to posterior dislocation at the knee joint or laceration of popliteal fossa leads to dorsiflexion and eversion of foot. |
| • |
Baker’s cyst—inflammation of bursa deep to semimembranosus. |
| • |
Pulsations of popliteal artery can be felt on deep palpation just medial to the midline against the popliteal surface of femur in a partially flexed knee. |
|
